Treatment
The earlier a lazy eye is detected the better. Once the development stage for the eye is over no further improvement can be attained, so the treatment must commence as soon as possible.
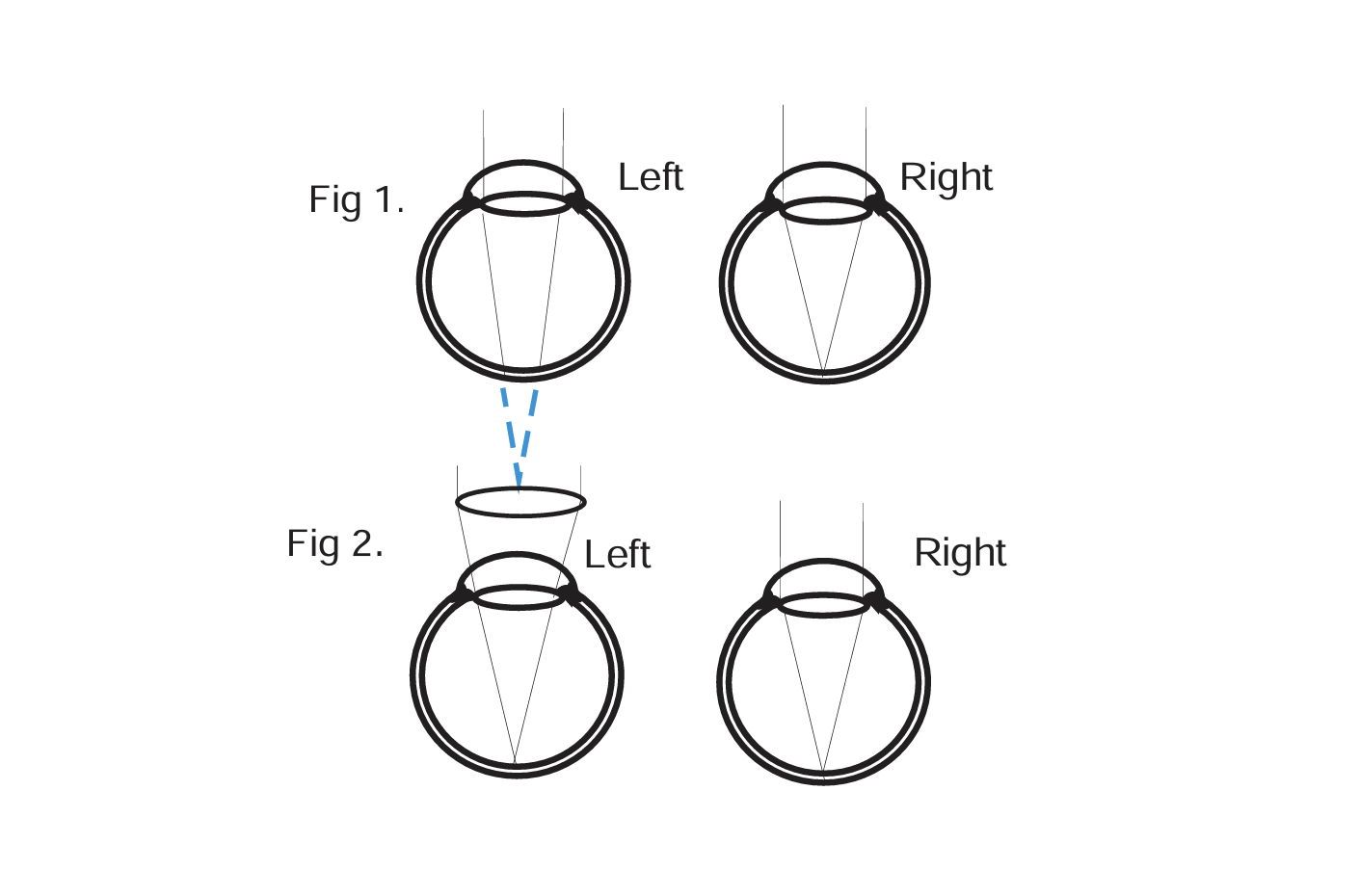
Firstly the reason for the blurred retinal image has to be managed. A refractive problem would require immediate spectacle correction (Fig 2) to ensure both eyes receive clear retinal images. In this situation the child may not feel the spectacles improve vision. This is because the child’s eye dominance is toward the non lazy eye which may not require any spectacle correction at all. Furthermore, the power of the strong spectacle lens may actually make the glasses visually uncomfortable to wear. Regardless of this the child must wear the glasses all the time to maintain constant foveal stimulation. Parents may find it difficult to ensure constant wear when the child does not feel comfortable in the glasses and does not perceive a visual improvement with them. If the problem is not purely refractive and there is an eye turn involved as well, then referral to the ophthalmology department would probably be necessary to surgically straighten the eye.
Often, if caught early, spectacle correction alone will be sufficient to correct amblyopia. Sometimes, however, the non lazy eye may be patched to further stimulate the poor eye to be used. Patching no longer needs to be constant. Short, intense patching often gives excellent results - perhaps two hours per day while the child does a visually taxing task such as drawing or reading. This can be a preferable strategy since the child will not be seen with the patch and he/she will not be forced to use the poor eye at school when optimal vision is important.
If patching is to be tried it is usual to patch the eye itself, rather than the spectacle lens, otherwise the child may peer around the patch. There is a need to be adaptable though, since not all children accept the strategy and it is sometimes necessary to modify the plan if the child is non compliant.
Very regular checks are essential if amblyopia training is to be undertaken. First, to assess improvement. We like to show parents the level of vision for their child on the eye chart before and during treatment. This helps the parents appreciate any improvements as they are achieved. Secondly, to ensure both parents and children are compliant with the strategy. If there seems to be a problem then we may need to modify the plan to suit the situation. It is not uncommon initially for checks to be at monthly or three monthly intervals. Flexibility in the assessment schedule is again essential if results are not straight forward.
Ideally we would continue treatment as long as improvements in vision are noted and as long as the parents and child remain compliant and keen. Initial improvements can be quite marked and then gradually taper off. The end point of treatment tends to be when, after several consecutive visits, no further improvement is noted.
Conclusion
Once the sight is improved as much as possible, and once the elastic period of eye development is past, spectacle wear becomes less stringent. At this stage the optometrist may suggest the child wear the glasses less or cease wear altogether. This does not mean the refractive error has disappeared, simply that with both eyes open the child may not notice any visual difficulties. Continued wear depends, to a degree, on what the patient says. If the child likes wearing the glasses and feels more comfortable with them, then we would continue to prescribe them. However, if the child does not report a qualitative improvement with the glasses, and if other factors are not of concern, then wear can be reduced or stopped. Annual reviews would still be recommended to monitor general ocular health.



.jpeg)
